Mass and/or mandatory vaccination of children with unproven experimental COVID injections has very low, if any, benefit to healthy children who rarely become infected. The risk of adverse events is very substantial.
Parents and children are emotionally manipulated into believing that the child ‘vaccine’ will ‘protect’ grandma and grandpa, when the risk of transmission from asymptomatic children is zero or extremely negligible. Children are being asked to sacrifice their lives for the sake of the elderly.
We are moving towards approval of mass vaccination of our children with an experimental inoculation which does not stop infection or transmission. ‘Protection’ is unproven. Injury and death rates to children are unknown. The risks may be substantial. The benefits to children are very low or perhaps non-existent.
What is this doing to children’s psyche? We are introducing fear of contagion, and restricting and interrupting their childhood learning and socialisation. Some children may feel guilty that they are stopping their parents going to work, and fearful that they could become responsible for hurting grandma and grandpa.
If a mother tests positive then her children are ‘close contacts’ and all their classes and their teachers must be PCR tested and isolate until the results are known.
These ‘COVID safe’ mandatory policies are disrupting working parents incomes and jobs, children’s education and teachers careers and incomes in an unpredictable, random and chaotic way.
Tracking, tracing, testing, isolating and quarantining is impacting mental and physical health, wellbeing and learning of children as well as incomes and job security of parents.
Widespread PCR Testing of school children may produce false positives of 80% plus which in turn may build the support for ‘Provisional Approval’ (in Australia) or ‘Emergency Use Authorisation’ (In America) of experimental mRNA and DNA injections.
Children have substantial dangers from COVID vaccines of long-term reduction of natural immunity, as well as injury and death.
Why on earth would we contemplate mass, and possibly mandatory COVID vaccination of children?
This is an extract of Geert Vanden Bossche’s interview with Doctors for Life Philippines, where he talks about the importance of the natural immune system for children, and why mass vaccination in children is unforgivable.
“A new study from Germany showed extremely few deaths among healthy children overall — including zero deaths among children 5 to 11 — suggesting some studies are designed to distort the risk to kids.”
Bill Gates’ Gavi Vaccine Alliance in 2018 published a paper on itsINFUSE programthat ought to be required reading for every parent of young children.
This document is guaranteed to give pause to any parent considering taking the advice of Dr. Anthony Fauci, their local public-school nurse or government-compliant pediatrician who insists they get their child jabbed.
So is there another explanation for why these diseases disappeared? The history of smallpox vaccination policy has been driven by ongoing fraud, force and folly.
Fraud:
Edward Jenner (1749-1823) is credited as the founding father of smallpox vaccination. He documented 23 cases where people who presented with what was diagnosed as cow pox, were later inoculated with smallpox, and appeared not to get the disease.
There was no comparative control group who didn’t get the inoculation.
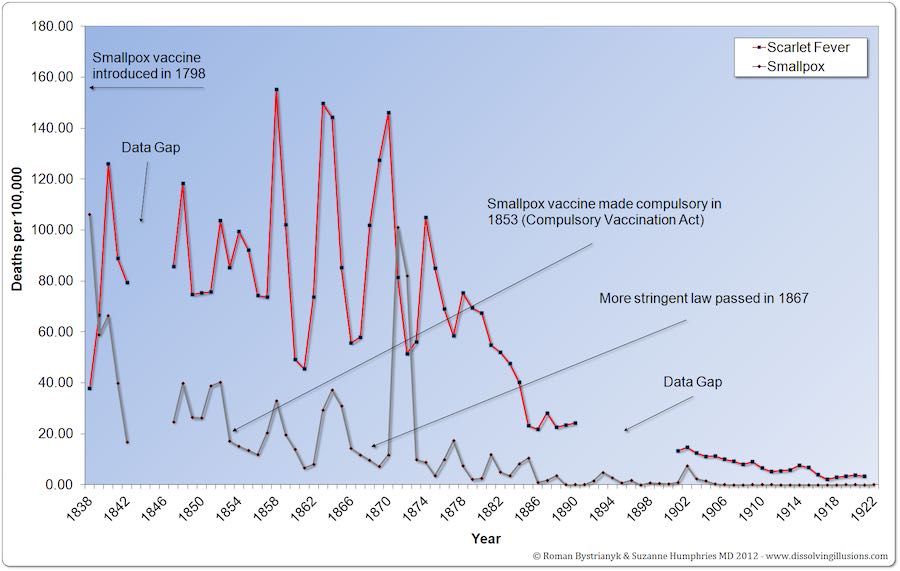
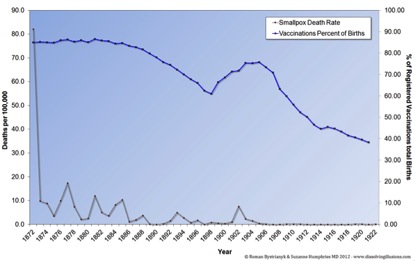
The greatest smallpox epidemic in Leicester (1870- 1874), coincided exactly with the period of greatest vaccination. Smallpox deaths declined thereafter even as vaccination rates plummeted.
On 23rd March 1885, what became known as the Great Demonstration against compulsory vaccination took place in Leicester, UK. The march of 100,000 people stretched for two miles.
That same year, the Leicester government was replaced with a new government opposing compulsory Vaccination. By 1887 vaccination coverage rate dropped to 10%.
“After this evidence that smallpox vaccination didn’t work, the people of Leicester in the English midlands refused to have the vaccine any more. When the next smallpox epidemic struck in the early 1890s the people of Leicester relied upon good sanitation and a system of quarantine. There was only one death from smallpox in Leicester during that epidemic. In contrast the citizens of other towns (who had been vaccinated) died in vast numbers…Doctors and drug companies may not like it but the truth is that surveillance, quarantine and better living conditions got rid of smallpox – not the smallpox vaccine.”– Dr. Vernon Coleman, MB
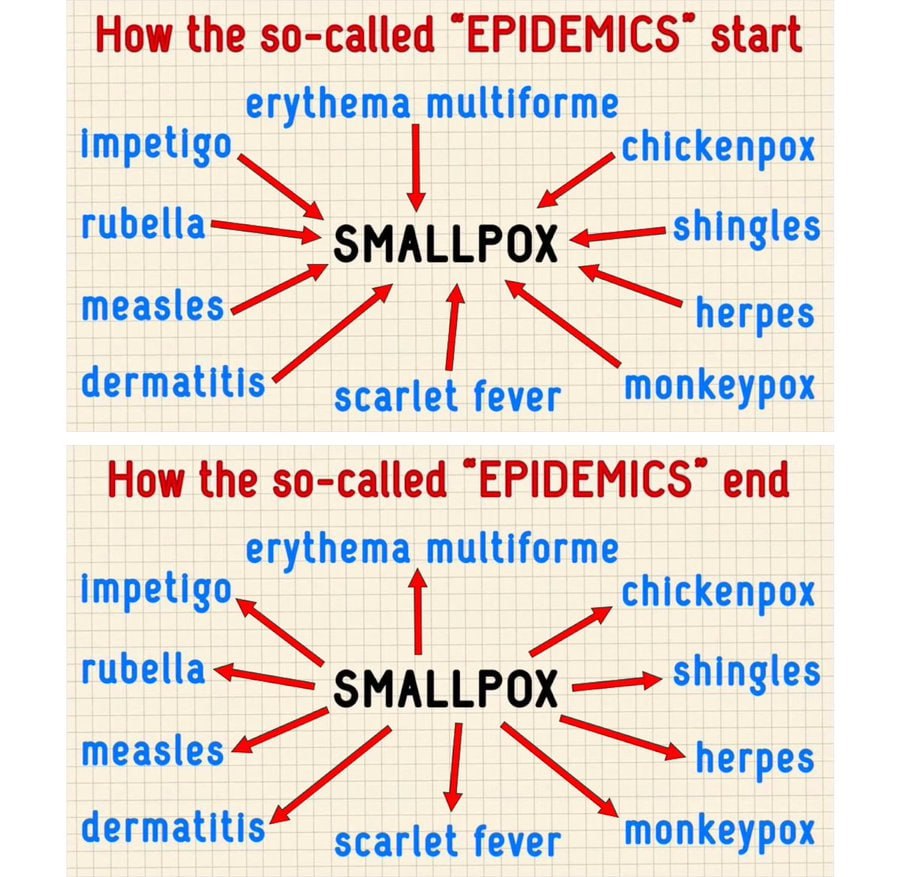
So how was the fraud maintained? A person who was vaccinated and then came down with the disease that they were supposedly “protected” against, was simply recorded under another name. From 1904 to 1934 in England and Wales, 3,112 died of chicken pox and 579 died of smallpox according to the health records. In other words, people who have been vaccinated for smallpox and had later come down with the disease were classified in the health records as having chickenpox.
Using this strategy, the WHO started its campaign to eradicate smallpox in 1958, in the same year they named an infectious disease monkeypox. According to the WHO, the disease was clinically indistinguishable from smallpox. This correlates well with the findings of George Bernard Shaw:
Monkeypox is still an active disease today. By claiming a monkey could be a vector they hid the fact that the smallpox could be the cause of the infection. This was the basic framework for the Global Smallpox Eradication Campaign. Over the past 20 years ten Central and West African countries have reported that monkeypox cases have risen exponentially.
The last reported case of death from smallpox, was the medical photographer, Janet Parker, in 1978. Conspiracy surrounds the case. Her father died of a heart attack in quarantine. Her mother supposedly contracted smallpox after being vaccinated and the head of the lab, were Janet had been employed, committed suicide by cutting his own throat. As a result of this case, the WHO instructed labs to destroy their smallpox stock. It was suggested that the existence of these labs posed a threat to the success of the Global Smallpox Eradication Campaign.
The WHO has subsequently used the myth, that smallpox had been eradicated, to give credentials to the whole vaccine program worldwide. Most people now believe that vaccines have saved us from the most dreaded infectious diseases. They have no idea that the real decline in infectious disease deaths was due almost entirely to improved sanitation, clean drinking water, nutrition and higher living standards.
Force
In the UK in 1840, as doctors and citizens realized that smallpox vaccination was not what it was promised to be, vaccine refusals increased. Governments passed various laws to force people to be vaccinated.
The compulsory vaccination law was repealed in 1907. By 1919, England and Wales had become one of the least vaccinated countries and had only 28 deaths from smallpox out of a population of 37.8 million people.
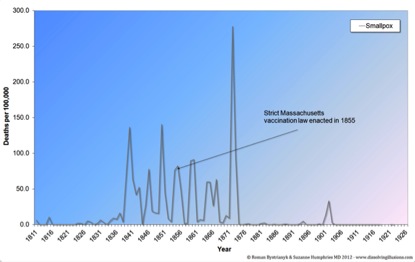
Massachusetts, USA, in 1855, took the most advanced stand ever taken by any of the states and enacted a law which required parents or guardians to cause the vaccination of all children before they were two years old, and forbade the admission of all children to the public schools of any child who had not been duly vaccinated. Parents who did not vaccinate their children by age 2 faced a fine of $5 yearly (about $156 in today’s dollars).
New Jersey, 1906, 30,000 pupils and teachers were forced to submit to vaccination. Twenty teachers and hundreds of pupils who refused, were suspended. Many of those vaccinated became seriously ill.
To maintain the prestige of the medical profession and themselves, the government put the full force of their powers to legislate compulsory vaccination. They used public funds and the power of the police to enforce inoculations on the unwilling and defenseless.
Folly
“Smallpox vaccination has always correlated positively to epidemics in the countries that collected data in the vain hope of proving the vaccine’s worth.” Dissolving Illusions” by Suzanne Humphries, MD and Roman Bystrianyk
In Leicester, UK, reports of deaths and outbreaks created doubts about the effectiveness and safety of vaccines. There was a growing list of complications attributed to vaccination. The 1871-72 smallpox epidemic provided a vivid example to the townspeople, as some 3,000 cases occurred and of these 358 died. Some of those dead had been vaccinated according to the law.
In Boston, the same situation was occurring. Massachusetts data began in 1811 and showed that, starting around 1837, there were periodic smallpox epidemics. Following the 1855 mandates, there were smallpox epidemics in 1859–1860, 1864–1865, and 1867, culminating with the infamous epidemic in 1872–1873. These repeated smallpox epidemics showed that the strict vaccination laws instituted by Massachusetts had no beneficial effect.
Smallpox deaths in children under 5 yrs = 8, Sp. vaccination deaths = 30
Smallpox vaccines were proving themselves to be neither safe nor effective. Epidemics were increasing in severity in the wake of vaccination. Correspondingly, they were decreasing as vaccination rates declined. Improved living conditions were having a better effect and had all but wiped smallpox out.
With exquisite irony, a 1972 smallpox outbreak in Yugoslavia was halted through use of the Leicester Method. This involved rapid quarantining of cases and contacts, as well as, cleaning of the houses. – while the authorities vaccinated 18 million citizens in full knowledge of its ineffectiveness. Vaccination had to be implemented if the story of ‘vaccine success’ was to be upheld.
The folly was always, the belief that you could safely inject some infective agent, of highly dubious toxicity, into the body of a healthy individual, or a really seriously unhealthy individual. This was to prevent, or mitigate the severity of, an illness that was already reportedly mild in most developed nations, or in many countries non-existent.
The risk of contracting the illness had to be outweighed against the risk of the vaccine. Taking the vaccine into your system, exposed you to all the potential side effects, including serious injury and death.
The only way this scenario could ever be accepted was to deny alternative methods and alternative policies, censor any knowledge of adverse events, and ‘discover’ an illness almost identical, and name it ‘monkeypox’.
The legacy of the smallpox story lives on in our understanding and acceptance of vaccines today. “Vaccines save lives and adverse events are rare” still frames the belief system driving vaccine compliance.
Vaccination programs and antibiotics have mistakenly been given all the credit for declines in killer diseases such as smallpox, cholera, typhoid, tuberculosis, dysentery, etc. Most or all of the credit belongs to better hygiene, sanitation, housing, and greater resistance to disease thanks to improved economic conditions and better nutrition.
In fact, many keen observers commented that it may have been because of how OBVIOUS it had become that the smallpox vaccines were spreading smallpox, that the WHO (World Health Organization) was motivated to cease the vaccination program but credit it for the eradication!
Has smallpox been eradicated? Was it eradicated from laboratories? What does Bill Gates say about the global future of smallpox?
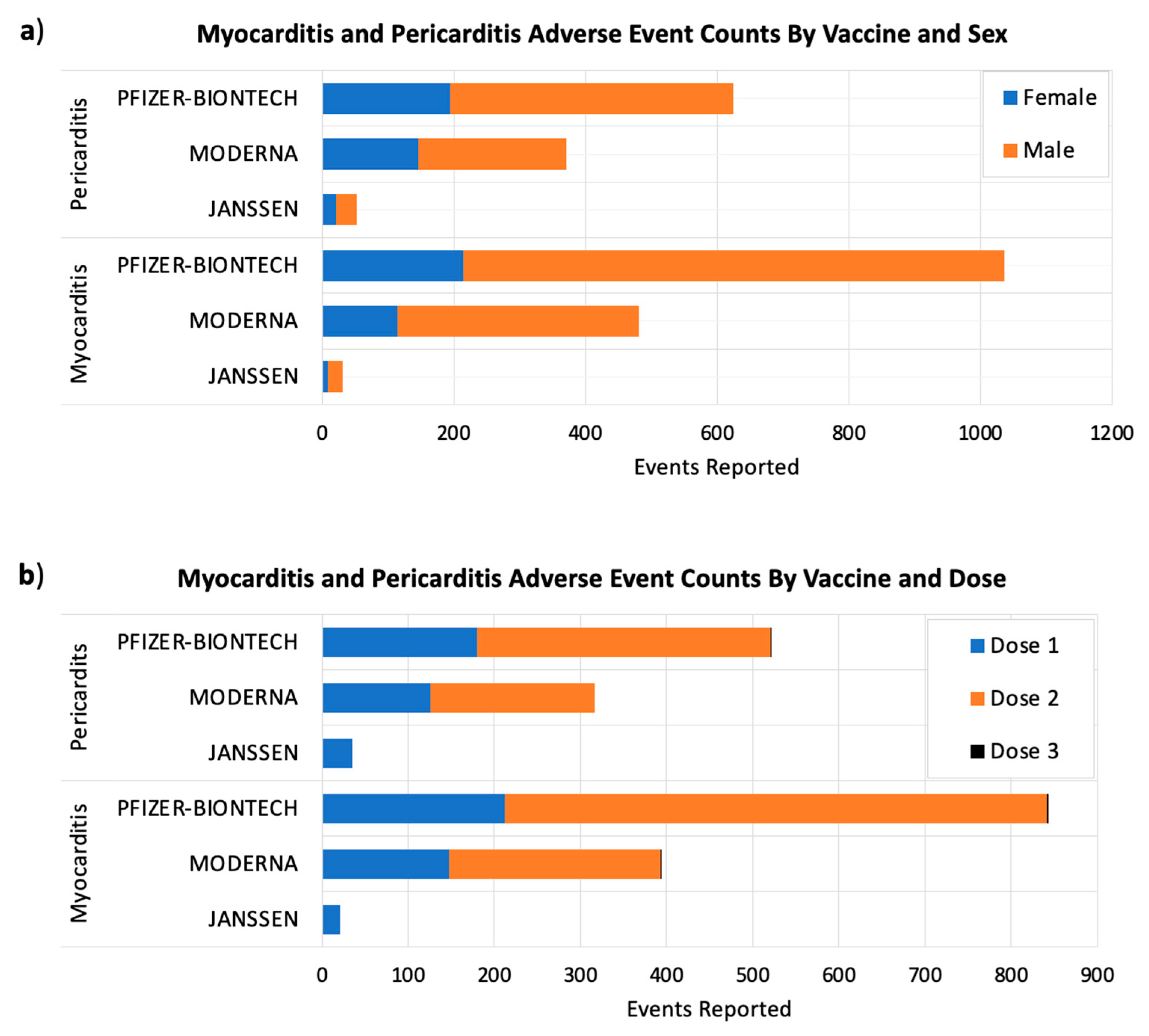
The CDC admitted that 1 in 175 recipients of the ACAM2000 vaccine (which the buyers had hoped would be safer than the older Dryvax vaccine) developed myocarditis. If you consider that every military service-member had to receive a smallpox vaccine starting in 2003 (and prior to the early 80s) , there could have been up to 50,000 cases of vaccine-induced myocarditis.
We are a large and ever growing group of Americans who were previously healthy and have been seriously injured by the COVID vaccines (Pfizer, Moderna, J&J as well as Astra Zeneca in the clinical trial stage in the United States).
In a study published June 29 in JAMA Cardiology, researchers described 23 cases of myocarditis in healthy military members who developed the condition within four days of receiving the Pfizer or Moderna COVID vaccines.
It comes from the AGAPLESION Bethanien Havelgarten retirement home in Berlin-Spandau. There, within four weeks after the first vaccination with the BioNTech/Pfizer vaccine Comirnaty, eight of 31 seniors, who suffered from dementia but were in good physical condition according to their age before the vaccination, died.
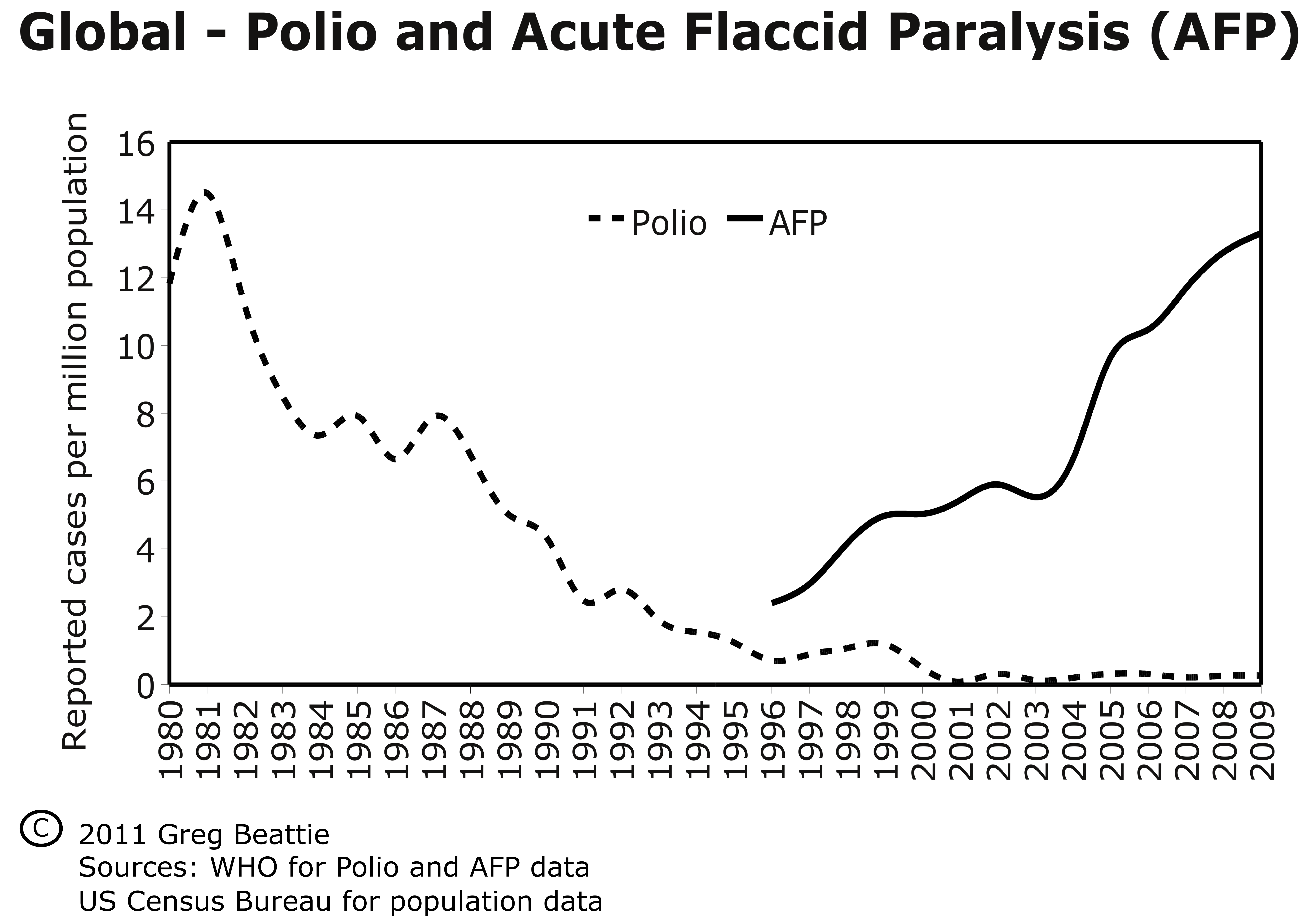
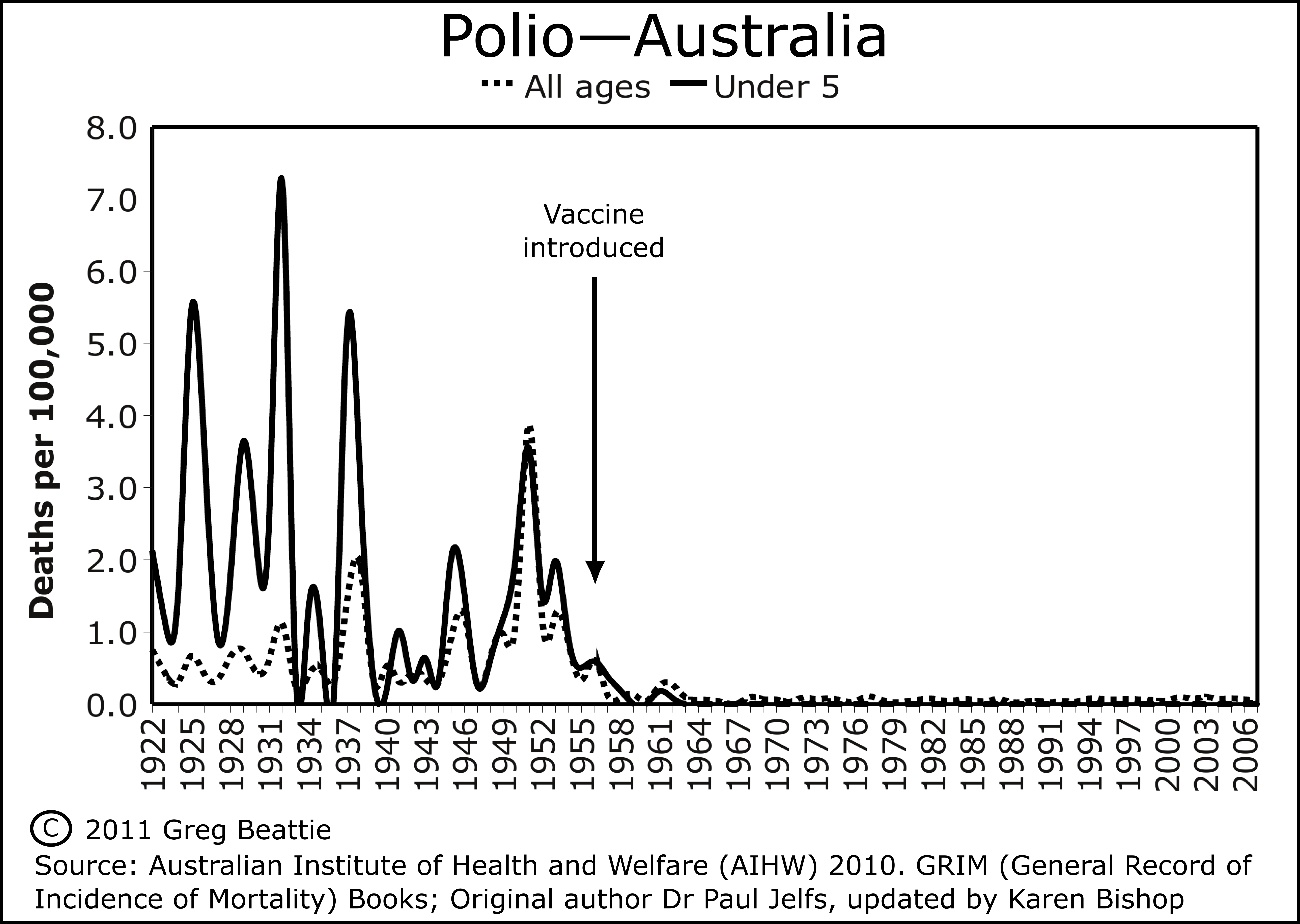
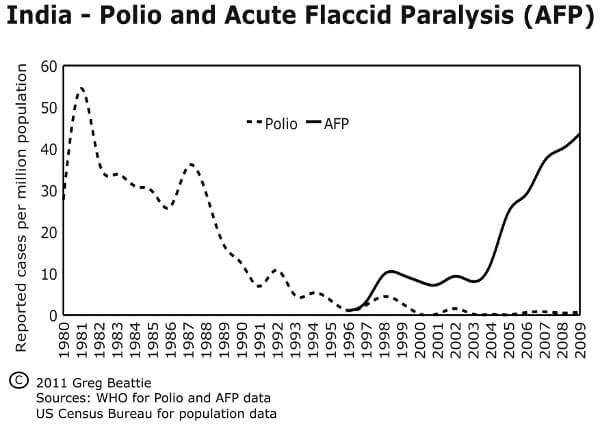
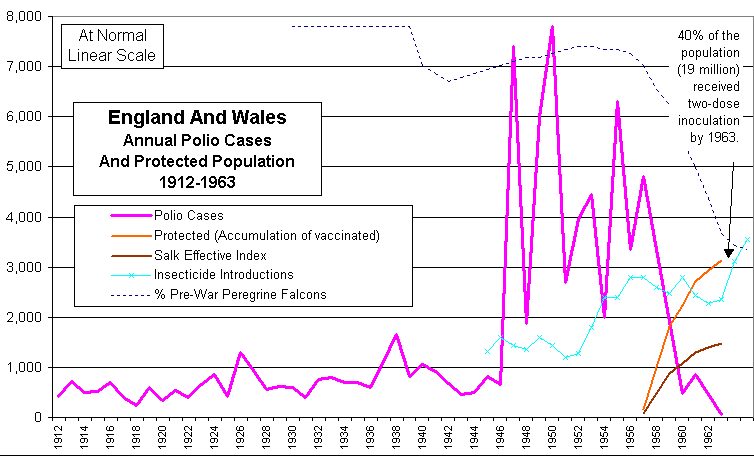
Inevitably, this is the first reason brought up in conversation to explain why vaccines are essential. The image immediately conjured up is of iron lungs and calipers on poor defenseless children in a hideous epidemic. The vaccines of Sabin and Salksupposedly led us to freedom from this dreaded illness.
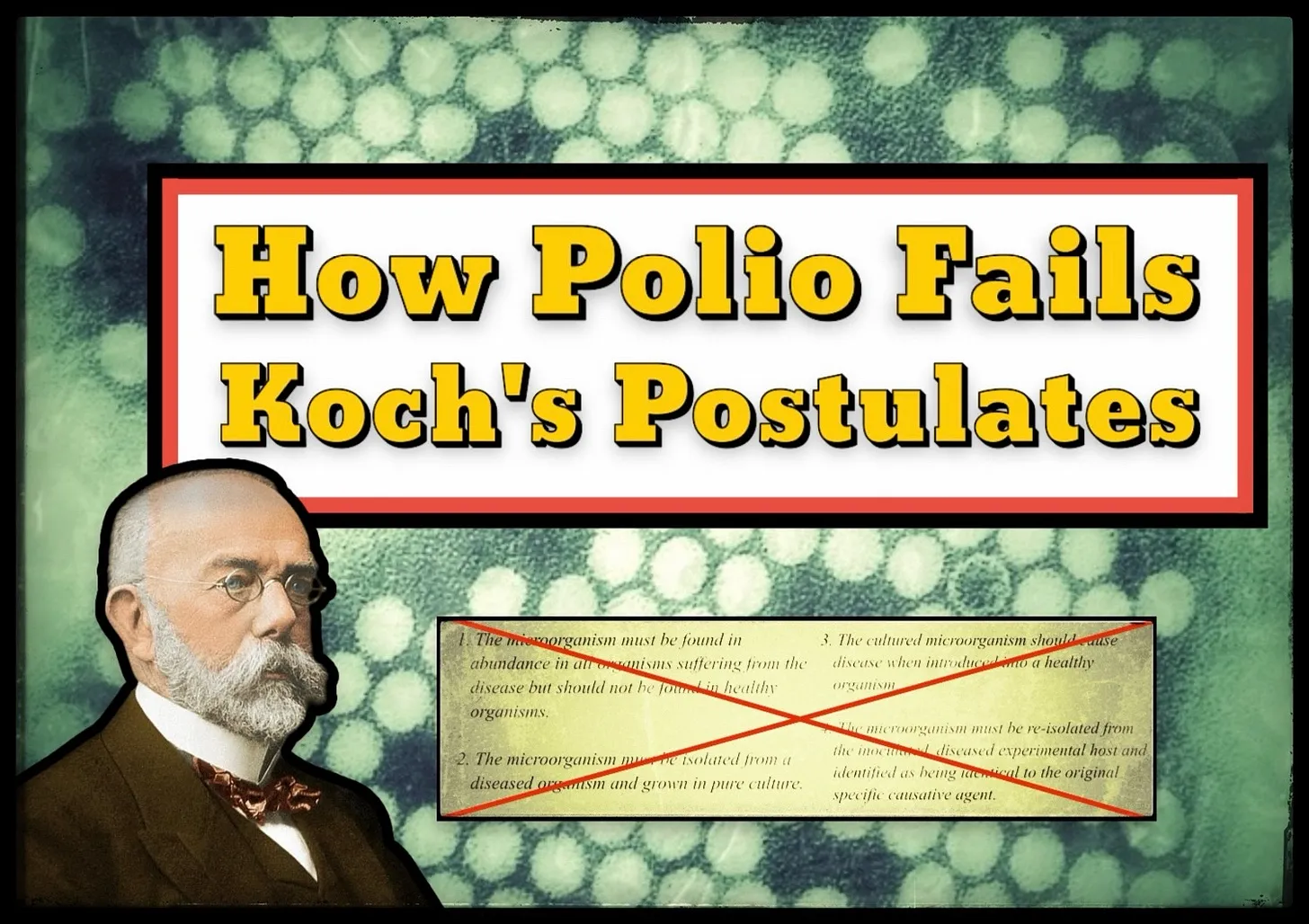
In the late 1800s, German bacteriologist Robert Koch developed four postulates, which outline a set of logical criteria necessary to establish that a microbe causes a specific disease.
They emphasize association, isolation, causation, and re-isolation. While phrased slightly differently in various sources, the postulates are most commonly stated as follows:
The microorganism must be found in abundance in all cases of those suffering from the disease, but should not be found in healthy subjects.
The microorganism must be isolated from a diseased subject and grown in pure culture.
The cultured microorganism should cause the same disease when introduced into a healthy subject.
The microorganism must be reisolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent.
Postulate 1: The microorganism must be found in abundance in all cases of those suffering from the disease, but should not be found in healthy subjects. – “During an epidemic of poliomyelitis in Michigan in 1958, virological and serologic studies were carried out with specimens from 1,060 patients. – Fecal specimens from 869 patients yielded no virus in 401 cases, poliovirus in 292, ECHO (enteric cytopathogenic human orphan) virus in 100, Coxsackie virus in 73, and unidentified virus in 3 cases. – Serums from 191 patients from whom no fecal specimens were obtainable showed no antibody changes
Postulate 2: The microorganism must be isolated from a diseased subject and grown in pure culture.
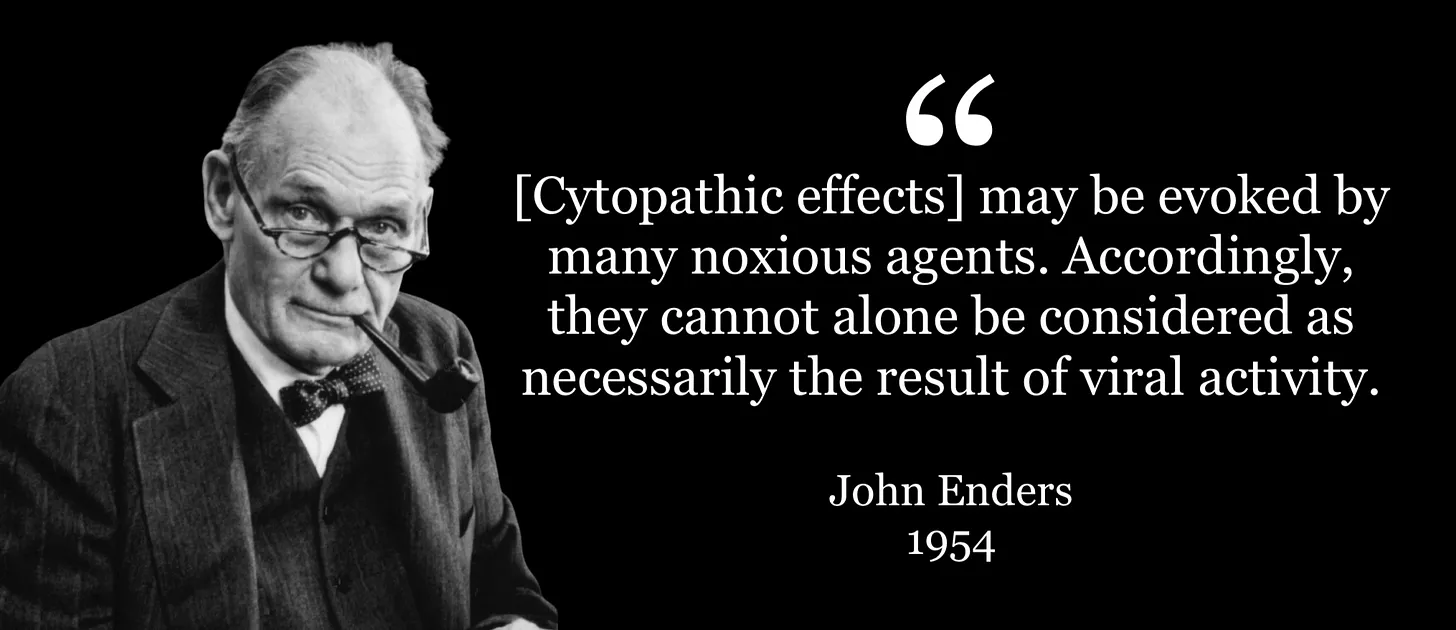
In 1949, a man named John Enders developed a technique for allegedly cultivating the polio “virus” in vitro. He observed some chemical reactions in a cell culture, and proclaimed that a virus was present.
However, such a procedure does not represent the isolation of a pathogen in a pure culture, as acknowledged by virologistJoseph L. Melnickin 1951.
“There is as yet no clear evidence that the [polio] virus has been obtained in pure form”
Ender’slater admitted that these lab-created effects could not be “considered as necessarily the result of viral activity.”
Many of the leading light doctors who courageously spoke out and did ground-breaking research during the COVID plandemic , nevertheless made it clear publicly that, in general, they believed vaccines to be ‘safe and effective’ whereas the mRNA technology was exceptionally harmful and ineffective , and even of negative efficacy within months. The Midwestern Doctor has presented important evidence showing that we need to be wary of claims that ‘traditional’ vaccines are generally safe and effective.
” We have identified a chronic enterocolitis in children that may be related to neuropsychiatric dysfunction. In most cases, onset of symptoms was after measles, mumps, and rubella immunisation. Further investigations are needed to examine this syndrome and its possible relation to this vaccine.”
In part 1 and part 2 of this series, we discussed the HPV vaccine and its links to ovarian insufficiency and autoimmune disease. In part 3, we turn to questions regarding the effectiveness of the vaccine to prevent cervical cancer, and the limitations of relevant clinical trials to detect such a type of effect.
In this HPV vaccine series, Parts I and II explain how the vaccine works and the evidence suggesting there may be legitimate safety concerns. The remaining parts present questions about real-world vaccine effectiveness and identify specific ingredients which may pose harm.
Vaccination is unjustified if the vaccine carries any substantial risk, as healthy teenagers face little to no risk of dying from cervical cancer. Risk-benefit analyses must be conducted to ascertain the overall balance of benefits and harms on both individual and societal levels.




 (see page 15)
(see page 15)